ExoSurge® Peyronie's Treatment Technology

Other Peyronie's questions?
What is ExoSurge technology and how does it work?
ExoSurge technology was born from over twenty years of focused research and collaborations. The first decade was dedicated mostly to uncovering what actually causes Peyronie’s (the epidemiology of Peyronie’s disease). We hypothesized we were unlikely to find a curative solution to the problem until we understood exactly what the problem was.
It’s long been hypothesized Peyronie’s is caused by penile trauma but that never explained many cases, including the most common version where otherwise perfectly healthy men simply awake with an ugly curve during morning erections. The ExoSurge team unlocked those secrets. Subsequently, they had to develop a treatment technology that could effectively remove the penile fibrous plaques that cause all Peyronie’s awful symptoms. Peyronie’s fibrosis is embedded in the penile neurovascular nerve bundle, making it impossible to effectively remove surgically without causing tremendous risk to lost sensation.
Following is an encapsulation of this new Peyronie’s technology.
ExoSurge® Inter-fibrinous Pulsated Gas and Drug Technology (IPG)
Introducing a paradigm-shift approach to treatment of Peyronie’s Disease.

How does ExoSurge work?
ExoSurge is a tandem of treatments guided by a detailed algorithm that results in safe dissolution of Peyronie’s fibrous plaques, which are the underlying source for the nasty symptoms Peyronie’s is famous for.
The key workhorse of this technology is the patented IPG pulsated gas injections which allow injected drugs to properly penetrate dense fibrous plaques and begin dissolution. In some cases (20%), we prescribe therapies to induce increased penile blood flow (if it’s found to be deficient) during ultrasound testing. All patients are put on regimens to optimize and improve their scoring with “Peyronie’s Accelerators”. Otherwise, the removal of fibrous plaques can be incredibly slow since the body is suited to add more when these metrics are out of alignment.
Eight issued patents, 18 patents and provisionals filed both nationally and internationally

Retrospective Study Results
Outcomes of Non-Surgical Treatment for Peyronie’s Disease: Retrospective, single clinic, observational cohort study
By:
Steven L. Morganstern, MD
Kenneth J. Carney, MD, PharmD, FACS
Angela Bates, APRN
Abstract
Objectives: The goal of this study is to evaluate the outcomes of a non-surgical treatment for Peyronie’s Disease.
Peyronie’s Disease (PD) is recognized as a difficult disease to treat within the medical community. The basis for difficulty may stem from the controversy in agreement on the etiology of PD (Nehra, et al., 2015). Most treatments to date are centered around treating the symptoms caused by the disease or for discouraging the initiation of fibrosis (Fallo & Sarnacchiaro, 2019) (Gonzalez-Cadavid & Rajfer, 2010). At this time there is only one treatment approved by the FDA (U.S. Food and Drug Administration) for non-surgical intervention of PD, clostridium collagenase histolyticum (CCH). This treatment can be effective however due to stringent qualifications for use, many patients suffering with PD are excluded from this treatment (Nehra, et al., 2015). Recommendations for treatment from the American Urological Association (AUA) include several options for medication usage with varying degrees of expected success, other than CCH. The evidence listed for these medications is rated as Grade C. This level of reliability in the research shows an expectation toward change in the confidence level with further research (Nehra, et al., 2015).
Materials and Methods: Of the 101 subjects reviewed, 31 patients were excluded due to a lack of continuity in record keeping leaving 70 patients who were actively in treatment between the dates of January 1, 2018 and March 6, 2020. Peyronie’s treatment using Exosurge follows current guidelines provided by the AUA for Peyronie’s Disease (Nehra, et al., 2015). No patients were excluded for past medical history, fibrotic condition of calcification, degree of initial curve or previous treatments.
Results: Changes in presentation after treatment resulted in 84% of patients with improvement. Of these patients, there was a 58% average reduction in curvature. Fourteen percent showed no change and only one patient worsened after treatments began.
The average plaque reduction was found to be 79%. Patients who had an initial curve showed an average plaque reduction of 88%. An incidental finding revealed that only 24% of patients with a curve greater than or equal to 30 degrees measured an acceptable erection grade of 3.5 or 4.0 at baseline. After treatments, this number increased to 42%.
Conclusion: Not only do these results show an impressive reduction in plaque size and consistency, but a notable difference was seen in the degree of curve and erectile function. This author feels there is enough evidence presented within this review to proceed to clinical trials for the use of ExoSurge as a foundational, non-surgical treatment for Peyronie’s Disease.
Key Points:
· 84% of patients showed improvement in their curve.
· 58% average reduction in curve.
· 79% overall reduction in plaque.
· 55% of patients with an initial curve greater than 30 degrees achieved an erection grade of at least 3.5 after treatment. This is an increase of 31%.
Outcome of Non-Surgical Treatment for Peyronie’s Disease:
Retrospective, single clinic, observational cohort study
Introduction
Peyronie’s Disease (PD) has been defined as a disease of the tunica albuginea in which fibrosis and plaque formation alter the physiology of the corpus cavernosum. The presentation of this plaque may cause a singular or a combination of changes such as erectile dysfunction, pain, curvature, reduction in girth and length as well as a “wasting effect” of the penis (Hussein, Alwaal, & Lue, 2015). During a systematic review performed by the AUA (Nehra, et al., 2015), a definition of PD was constructed as an abnormality characterized by fibrosis. Further, it was reported that PD may include pain, erectile dysfunction, or a deformity. Although symptoms are included in the definition of PD, it should be recognized that the base definition of PD is fibrosis.
Treatment for PD is controversial as most treatment modalities have minimal success and few show a continued progress toward resolution. Many known treatments only address the symptoms that present with PD and do not look to the cause. The AUA recommends that clinicians should only offer treatment if the clinician is experienced to treat the condition (Nehra, et al., 2015). The purpose of this study was to review the outcomes of PD patients undergoing the non-surgical treatment, ExoSurge at a single clinic, Morganstern Urology Clinic (The Clinic) between the dates of January 1, 2018, and March 6, 2020. No patients were excluded based on past medical history or type of treatment received in the clinic.
2 Method
2.1 Eligibility criteria for participants
A database search using The Clinic’s Electronic Health Records (EHR) system was completed extrapolating patient medical charts with the diagnosis of PD and undergoing treatment between the dates of January 1, 2018, and March 6, 2020. Patient charts were included when they were found to have identifiable and measurable plaque with no less than two duplex doppler ultrasound diagnostic tests within that timeframe providing a pre-treatment ultrasound and a post or intra-treatment ultrasound for comparison. Of these patients, 101 were found to be consistent in receiving treatments during this timeframe. Those excluded were patients who had not been seen in the clinic within three months or more prior to the post or intra-treatment ultrasound tests and considered inconsistent with treatment.
Upon further review it was determined that within this patient sampling of 101, some pre-treatment recordings of the duplex doppler ultrasound diagnostic test was not complete and/or not comparable in recording to the post and/or intra-treatment ultrasound and therefor were not considered a good comparison. These patient charts were removed from the study leaving a total of 70 patient charts for comparison. All duplex doppler ultrasound diagnostic testing during the listed dates was completed by an independent, outside source on site at The Clinic.
2.2 Past Medical History
Past medical history (PMH) for each patient was recorded only. No participants were excluded based on PMH. Past medical history was broken down into these categories: Cardiac, Diabetes Mellitus (DM), Cancer (CA), Cerebrovascular Accident (CVA) and Low Testosterone (Low T). The heading of cardiac included patients with diagnosis and having been medically treated for hypertension (HTN), hypercholesterolemia, arrhythmia, congestive heart failure (CHF) or had a history of myocardial infarction (MI). Patients were included in the diabetes category if they were found to have a history of being treated medically or were currently being treated for diabetes mellitus (DM).
2.3 Study Design
This was a single clinic, descriptive study conducted in review of clinical treatments by Morganstern Urology Clinic including patients undergoing treatment for Peyronie’s Disease between January 1, 2018, and March 6, 2020. Patient identification information was removed to maintain HIPAA Compliance.
Data retrieved from each duplex doppler ultrasound included degree of curve, identification of venous leak, identification of arterial insufficiency, erection grade, size of plaque, and consistency of plaque as either calcified or non-calcified.
2.4 Treatment Description
ExoSurge treatment includes a gas combined with an intralesional injection of no less than 1 mL of the calcium channel blocker verapamil. Other supportive treatments were used based on each patient’s individual presentation, but ExoSurge and Verapamil were administered to every patient in this study. Supportive treatments may have included straight stretching devices, vacuum devices, oral medications, intralesional medications and/or over the counter supplements.
2.5 Data Review & Analysis
A beginning baseline duplex doppler ultrasound analysis that included up to three measurable pieces of plaque was compared to a follow up duplex doppler ultrasound for measurable changes. Data retrieved from both the initial and final duplex doppler ultrasounds included findings of plaque. Plaque size was recorded in a 3-dimensional format in millimeters. Consistency of plaque was recorded as calcified or non-calcified. Penile curvature was identified in degree of curvature, which was then divided into two classes: curvature greater than or equal to 30 degrees and a curvature less than 30 degrees.
Vascular integrity was recorded by review of arterial flow and/or venous leak. A simple A to B Ratio was used to determine level of integrity. The average value of Peak Systolic Velocity (PSV) was recorded per sides left and right. The average value of End-Diastolic Velocity (EDV) was also recorded by sides left and right. These results were then divided into Healthy, Moderate or Severe and noted as left and right. An A/B ratio greater than 20 was labeled as healthy, between 7 and 19 as moderate and less than 7 as severe. For final review only results shown to have Moderate or Healthy in both the left and right side were recorded as “unhealthy”.
Erection grade was recorded on a scale of 1 to 4 with increments of 0.5 based on the Erection Hardness Score (EHS).

Figure 1 EHS (Goldstein, et al., 2008)
2.6 Statistical Analysis
Of the total 70 patients reviewed, 50 were found to have a curve not considered as natural and developing later in life. All 50 patients were evaluated with color duplex doppler ultrasound for the following variables: penile plaque volume, calcified vs. non-calcified plaque, degree of penile curvature, and aspects of erectile function. Existing health conditions were noted but have not been used to score or further rate any changes in the level of disease for this review.
Plaque volume was measured, in mm3. To calculate the volume of the penile plaque, we measured three dimensions of each piece to determine the volume; V = length ×width × depth. Up to three separate pieces of plaque were recorded when present.
Degree of penile curvature was recorded during the initial and follow up duplex doppler ultrasound by use of a protractor. In many cases, but not all, pictures were provided with protractor showing measurement of current curve. Value of curve was accepted with or without confirmation picture.
Each duplex doppler ultrasound included an intra-cavernosal injection of 10 mcg alprostadil (Nehra, et al., 2015) administered prior to any measurements (Cavallini, Scroppo, & Zucchi, 2016). PSV was recorded every five minutes for a total of thirty minutes on both the left and right sides. For purposes of evaluation, PSV readings less than 30 were considered deficient (Gomez Varela, Mateos Yeguas, Rodriguez, & Duran Vila, 2020) and recorded as “arterial insufficiency”. EDV was also recorded in the same increments. It is commonly recognized that the EDV must be low to offer an effective veno-occlusive mechanism (Cavallini, Scroppo, & Zucchi, 2016). For evaluation, we considered readings >4 cm/sec as insufficient and this is labeled as “venous leak”. A simple ratio calculation of PSV / EDV provided the ratio between the two ratings.
3 Results
3.1 ExoSurge treatment changes in Plaque size
3.1A Plaque Area One Condition:
For the baseline duplex Doppler ultrasonography, the total number of pieces counted were 66. Of these, 52 were non-calcified and 14 were calcified. On the follow up duplex Doppler ultrasonography, the total number was 58. Of these, 48 were non-calcified and 10 were calcified. The reduction in the number of calcified plaque pieces was 28.6%.
3.1B Plaque Area One Measurement:
The total plaque size measured with the baseline duplex Doppler ultrasonography in Area One was 302.9 mm3 and the follow up duplex Doppler tally in Area One was 55.7 mm3, representing an 81.5% reduction in penile plaque for the 70 patients.
3.1C Plaque Area Two Condition:
For the baseline duplex Doppler ultrasonography, the total number of pieces counted in plaque area Number Two were 42 with the follow up study showing a total of 40. Of the original 42 pieces, 28 were non-calcified and 14 were calcified. On the follow up duplex Doppler ultrasonography analysis for plaque in Area Two, 32 were non-calcified and 8 were calcified, a 43% decrease in calcified plaque.
3.1D Plaque Area Two Measurement:
The average total size as measured from the baseline duplex Doppler for area two was 209.9 mm3 and the follow up results measured 63.4 mm3, representing a 70% reduction in penile plaque.
3.1E Plaque Area Three Condition:
For the baseline duplex Doppler ultrasonography, the total number of pieces counted in plaque Area Three were 22. The follow up duplex Doppler ultrasonography showed a total of 23 plaque pieces. Of the original 22 pieces, 15 were non-calcified and 7 were calcified. Data derived from the follow up duplex Doppler ultrasonography indicated 18 plaque fragments were non-calcified and 5 were calcified, representing a 28.6% improvement in the reduction of calcified plaque.
3.1F Plaque Area Three Measurement:
The total size as measured with the baseline duplex Doppler ultrasonography study for plaque in area three was 198.45 mm3 and the follow up duplex Doppler ultrasonography was 30.59 mm3, representing an improvement in the reduction of penile plaque of 84.6%.
Figure 2 Plaque Size Reduction
3.1G Combined Areas Condition:
The initial baseline number of calcified plaque pieces derived from duplex Doppler ultrasonography among all 70 patients in this study was 35. The follow up duplex doppler study showed the total number of calcified plaque pieces after treatment was 23. This shows a 34.3% reduction in calcified plaque pieces.
The non-calcified numbers increased from an initial count of 95 to the follow up count of 98. This is an expected finding as the calcified plaque will change to non-calcified before it is no longer measurable.
3.1 H Combined Areas Measurement:
The initial baseline plaque size total derived from duplex Doppler ultrasonography among all 70 patients in this study was 711.2 mm3. The follow up duplex Doppler ultrasonography was 149.7 mm3. The combined measurable penile plaque reduction for all areas was 79.0%.

Figure 2 Penile Plaque Size Reduction
3.2 ExoSurge treatment change in curve
A comparison was made between initial duplex doppler ultrasound and final/intra-treatment ultrasound as some patients were still undergoing treatments. Of the initial 50 patients with a curve, 36 of those patients also had a venous leak. Of the 50 patients with a curve, 17 of them had a curve less than 30 degrees with 12 of those with a venous leak. Thirty-three of the 50 had a curve greater than 30 degrees, of which 24 had a venous leak. The final study review of the 50 pts who were initially found to have a curve, 8 of those patients had no curve at all. Of the original 33 with a curve greater than 30 degrees, this number decreased to only 20 patients. On the initial study only 17 patients had a curve less than 30 degrees and this increased to 22. Therefore, 8 patients completely corrected to no longer have a curve and 5 had reduced significantly, one patient’s curve increased by 8 degrees. A 58% reduction in curve was noted for the entire group who showed a decrease in the degree of curve. Fourteen percent of patients showed no improvements with the curve.
During the time reviewed, we found only 24 patients still receiving therapy at the final date for review. The individual average improvement for these patients at the end date was 60%. Of the 26 patients no longer participating in treatment, there was an individual average improvement of 55% to their curvature. This change is congruent with our observations showing the largest change in curvature realized toward the end of therapy.
Figure 3 Improvements Average Per Patient
3.3 ExoSurge treatment changes in erectile dysfunction


Figure 4 EHS Patient Improvement
This study was a Peyronie’s disease/plaque study and shows reduction in volume of plaque however, the results may be easier to see when reviewing the changes recognized in the degree of curve. Of the total 70 patients reviewed, 16 were initially found to show an erection grade of 3.5 or higher. The data reviewed is the measured erections grade found on the first and last vascular study to allow for comparison. Initially, of the total 70 patients, 13 patients were evaluated at an erection grade of 4, after treatments there was a total of 16 patients. Initially only 3 pts were graded at a 3.5 but there was a total of 20 patients on the re-evaluation. It could be that those 3 patients who were graded at a 3.5 moved up to a 4 and the 20 came from patients who initially were found with erections grades at a 3 or lower. Therefore, to begin with only 16 patients had erection grades of 3.5 or 4 out of the original 70 participants but afterward 36 patients showed a grade of 3.5 or 4.
4 Discussion
Although this study was to review the success or failure of a new, non-surgical technique for correction of Peyronie’s Disease the data obtained has value in treatments for erectile dysfunction related to venous leak and arterial insufficiency. Further review is necessary to identify the variables and obtain a more in-depth presentation toward future treatment recommendations for ED. Within the cohort information collected for this review, there is sufficient data for other conclusions related to abnormalities of the penile shaft.
Many of the tools used during the initial and subsequent duplex doppler ultrasound studies were standardized to the industry however the A/B ratio used for review of PSV to EDV was not. It appears to be sufficient to identify venous leak levels in conjunction with arterial flow for this data review, however the Resistive Index (RI) is more common practice and should be evaluated for future use. Although the A/B ratio is used in The Clinic for determining different treatment options, it does not seem to directly correlate with erection grade.
Surprisingly, there appeared to be a connection with patients who initially showed a venous leak alone or in combination with arterial insufficiency and their original erection score. This data should be reviewed for analysis of vaso-occlusive erectile dysfunction.
Based on our findings, it would be of interest to review and compare each patients PMH along with their level of treatment to see to what degree these disease processes affect the treatment of Peyronie’s Disease (Herrera, Henke, & Bitterman, 2018) (Ming, Ma, Xhang, Guo, & Yuan, 2020) and not just the disease itself.
5 Conclusion
The review of data has shown significant improvements with patients undergoing ExoSurge treatments and Verapamil. This data proves this to be a successful foundational treatment for Peyronie’s Disease in patients of all conditions and medical histories. Not only did these results show an impressive reduction in plaque size and consistency, but a notable difference was also seen in degree of curve as well as erectile function. Current guidelines from the AUA for the treatment of Peyronie’s Disease include several options for treatment and a category named “Other Treatments”. Also included are recommendations for surgical intervention if a patient presents with erectile dysfunction along with PD (Nehra, et al., 2015). The results indicate that not only is there is enough evidence presented to proceed to clinical trials for the use of ExoSurge as a, non-surgical treatment for Peyronie’s Disease but also shows that improvements can be made in PD patients who experience ED as well. We should not be going directly to surgical intervention for patients with ED. This treatment continues to follow current guidelines provided by the AUA while avoiding recommended irreversible surgical interventions such as penile prosthesis or grafting.
5 Authors Notes/Conflicts of Interest
Authors are current members of the care team at Morganstern Urology and active during treatment administration, data assimilation and extrapolation.
References
Brock, G., Hsu, G., Nunes, L., von Heyden, B., & Lue, T. (1997, Jan). The anatomy of the tunica albuginea in the normal penis and Peyronie’s disease. Jurnal of Urology, 157(1), 276-81.
Cavallini, G., Scroppo, F. I., & Zucchi, A. (2016). Peak systolic velocity thresholds of cavernosal penile arteries in patients with and without risk factors for arterial erectile deficiency. Andrology. doi: https://doi.org/10.1111/andr.12242
Connolly, J. A., Borirakchanyavat, S., & Lue, T. F. (1996). Ultrasound evaluation of the penis for assessment of impotence. Journal of Clinical Ultrasound. doi:https://doi.org/10.1002/(SICI)1097-0096(199610)24:8<481::AID-JCU8>3.0.CO;2-G
Fallo, L., & Sarnacchiaro, P. (2019, April). Ten-year experience with multimodal treatment for acute phase Peyronie’s disease: A real life clinical report Ten years of experience with the multimodal treatment of the acute phase of Peyronie’s disease: real-life medical report. Spanish Urological Records (English Edition), Online 1-3. doi:10.1016//J.acuroe.2019.03.007
Goldstein, I., Mulhall, J. P., Bushmakin, A. G., Cappelleri, J. C., Hvidsten, K., & Symonds, T. (2008, Oct 8). The Erection Hardness Score and Its Relationship to Successful Sexual Intercourse. (10, Ed.) The Journal of Sexual Medicine, 2374-2380. doi:10.1111/j.1743-6109.2008.00910.x
Gomez Varela, C., Mateos Yeguas, L. A., Rodriguez, I. C., & Duran Vila, M. D. (2020). Penile Doppler Ultrasound for Erectile Dysfunction: Technique and Interpretation. American Journal of Roentgenology, 214(5), 1112-1121.
Gonzalez-Cadavid, N. F., & Rajfer, J. (2010). treatment of Peyronie’s disease with PDE5 inhibitors: an antifibrotic strategy. Nat Rev Urol, 7, 215-221.
Herrera, J., Henke, C. A., & Bitterman, P. B. (2018, 01 2). Extracellular matrix as a driver of progressive fibrosis. J Cli Invest, 128(1), 45-53. doi:10.1172/JCI93557
Hussein, A. A., Alwaal, A., & Lue, T. F. (2015). All about Peyronie’s disease. Asian Journal of Urology, 2, 70-78.
Lue, T. F., Kricak, H., Marich, K. W., & Tanagho, E. A. (1985). Vasculogenic impotence evaluated by high-resolution ultrasonography and pulsed Doppler spectrum analysis. Radiology, 155(3). doi:https://doi.org/10.1148/radiology.155.3.3890009
Ming, L., Ma, X., Xhang, X.-L., Guo, L.-Q., & Yuan, M.-Z. (2020). Significance of blood lipid parameters as effective markers for arteriogenic erectile dysfunction. Andrology, 8, 1086-1094. doi:doi.com/10.1111/andr.12776
Nehra, A., Alterowitz, R., Culkin, D., Faraday, M. M., Hakim, L. S., Heidelbaugh, J. J., . . . Burnett, A. L. (2015). Peyronie’s Disease: AUA Guideline. Journal of Urology, 194, 745-753. doi:10.1016
Padma-Nathan, H., Stecher, V. J., Sweeney, M., Orazem, J., Tseng, L.-J., & Deriesthal, H. (2003). Minimal time to successful intercourse after sildenafil citrate: results of a randomized, double-blind, placebo-controlled trial. Urology, 62(3), 400-403. doi:doi: 10.1016/s0090-4295(03)00567-3
Prajapati, D., Rampal, K., Ali, I., Rangera, M., Chaurisia, S., & Prajapati, J. M. (2016). Penile fracture and its managment. International Surgery Journal, 3(4), 1714-1717. doi:10.18203/2349-2902.isj20163552
Wynn, T. A. (2009, Jun). Cellular and molecular mechanisms of fibrosis. J Pathol, 214(2), 199-210. doi:10.1002/path.2277
Table of Figures
Figure 1 EHS (Goldstein, et al., 2008)
Figure 2 Plaque Size Reduction
Figure 3 Improvements Average Per Patient
Figure 4 EHS Patient Improvement
The ExoSurge Treatment Device
Our patented and clinically proven ExoSurge® method permanently removes fibrous tissue plaques linked to a Peyronie’s Disease diagnosis by using injected and pulsating gases in conjunction with intralesional medication injections.
A device roughly 24 inches wide by four feet tall that is mounted on rollers is used to administer these gas injections. As so, it may be rolled into place and stored in an exam room corner while patients are being treated. Before therapy starts, an initial assessment of the case dynamics is conducted, and interlesional injections of Trental, Verapamil, or both may be administered in combination with ExoSurge therapies.
The most frequent adverse effect is mild redness in the treated area, and treatments are well tolerated, taking approximately 15 to 20 minutes to complete. A single ExoSurge treatment per day is permitted for a patient.

What effects will this revolutionary ExoSurge technology have on Peyronie’s patients?
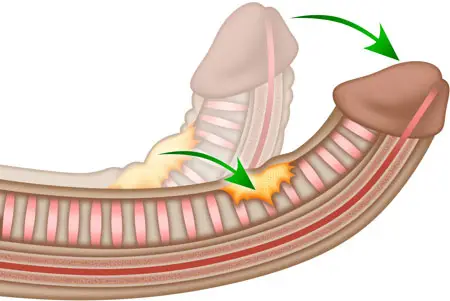
Erection-related penile curvature is a common indication of Peyronie’s disease. More than 60% of Peyronie’s cases include significant bending. The reason it happens most frequently is that the fibrous plaques that produce Peyronie’s symptoms typically develop along the tunica albuginea, which is the thick sheath that divides the erection tissue within the penis organ. If the left side of the tunica is where the majority of this fibrous plaque accumulation happens? When the penis is erect, it will curve to the left and, conversely, to the right. The degree of curvature is more prominent the larger the fibrous mass along the tunica.
However, curvature is only one of several common symptoms. It is not the root cause or definition of the condition.
When a disease remains incurable for centuries, its symptoms almost always become society’s definition of that disease.
Similarly, the efficacy of the treatments is measured by how well the symptoms are alleviated.
For example, this phenomenon is exemplified by the common cold. Coughing, sneezing, runny nose, sore throat and congestion are the most common symptoms, and people immediately assume we have a cold if we display these symptoms. Nobody inquiries about the type of virus we are fighting, such as rhinovirus, coronavirus, adenovirus, or enterovirus.
Since Peyronie’s Disease has remained similarly incurable, it has likewise become only known for its symptoms, even among many physicians, with erect curvature being the most notable definition. Thus, every approved treatment and medication for Peyronies is evaluated solely based on its efficacy in reducing erect curvature.

This is what makes ExoSurge® completely different from anything ever used to treat Peyronie’s.
ExoSurge® technology treats, heals and cures the underlying disease of Peyronie’s, not just its symptoms.
ExoSurge® is the world’s first clinically-proven treatment to conservatively and permanently remove plaques and fibrosis associated with a Peyronie’s diagnosis.
Our philosophy
Our clinic is focused on finding a cure for Peyronie’s Disease. After more than two decades of research and development, we’ve achieved many major milestones in pursuit of our purpose, including:
- We identified the underlying epidemiology of Peyronie’s.
- Our research identified six Peyronie’s Accelerators that need to be regulated and optimized to treat the disease.
- Our patented therapeutic uses pulsated gas injections to penetrate Peyronie’s fibrous plaques, allowing medications to breakdown fibrosis without surgery.
- Our new therapy algorithm takes into account all variables of a Peyronie’s case, such as plaque size, density, and position, as well as health factor rating and the state of each Peyronie’s Accelerator. This will assist future clinicians in treating cases.
Earlier in our Peyronie’s technology development, we were unable to restore the original size of the penis following the removal of Peyronie’s plaques, therefore we developed unique approaches for cosmetic urology (penis augmentation). Since then, we’ve learned ways to restore lost size from Peyronie’s during therapeutic treatments, but our cosmetic urology platform, led by renowned reconstructive urologist Kenneth J. Carney, MD, PHARM, FACS, has been highly successful. Our cosmetic platform has provided the principal funding for our Peyronie’s research.
We are now developing technology to accelerate the progression of obstinate Peyronie’s cases using enhanced techniques and innovative medications. We have initiated negotiations to partner with a multinational pharmaceutical platform to fund our FDA approvals and help ensure the ExoSurge breakthrough is available internationally in the coming years.